MKSAP Quiz: Evaluation for fatigue of 3 months' duration
A 36-year-old woman is evaluated for fatigue of 3 months' duration and dyspnea on exertion of 1 month's duration. She is 1 month postpartum. She takes no medications.
On physical examination, vital signs are normal. Pallor is noted. No scleral icterus is seen. The remainder of the examination is normal.
Laboratory studies:
Hemoglobin: 7.9 g/dL (79 g/L) (11.1 g/dL [111 g/L] in first trimester of pregnancy)
Leukocyte count: 6800/μL (6.8 × 109/L)
Mean corpuscular volume: 70 fL (80 fL in first trimester of pregnancy)
Platelet count: 414,000/μL (414 × 109/L)
Reticulocyte count: 1% of erythrocytes
Red-cell distribution width: Elevated
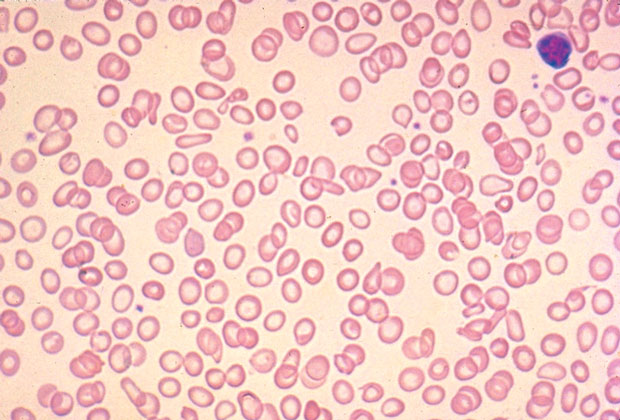
The peripheral blood smear is shown.
Which of the following is the most appropriate management?
A. Colonoscopy
B. Oral iron every other day
C. Oral iron three times daily
D. Hemoglobin electrophoresis
Answer and critique
The correct answer is B. Oral iron every other day. This content is available to MKSAP 19 subscribers as Question 59 in the Hematology section.
Beginning oral iron replacement therapy every other day is the most appropriate management option for this patient (Option B). A low mean corpuscular volume, elevated red-cell distribution width, and peripheral blood smear showing microcytosis and anisopoikilocytosis are virtually diagnostic of iron deficiency, especially in premenopausal women; these findings may obviate the need for additional laboratory testing provided that a follow-up blood count is performed to assess response to iron therapy. Even in developed nations, iron deficiency may be present in 20% to 30% of otherwise healthy women of childbearing age. Menstrual iron loss is the most common cause of anemia in this population. Iron deficiency anemia is also a common pregnancy complication because of the heightened iron requirements that occur in the second and third trimesters; it can be further exacerbated by inadequate oral iron intake because of nausea and vomiting. Iron deficiency is typically treated with oral iron salts. Frequent dosing (two or three times daily) of oral iron can lead to increased hepcidin production, which actually reduces iron absorption (Option C). For this reason, a single daily or every-other-day dose of oral iron sulfate may be the best replacement dose.
Gastrointestinal iron loss is a common cause of anemia in adults. Considering her age and lack of suggestive symptoms, this patient is more likely to have iron deficiency from menstrual losses before pregnancy and from the heightened iron requirements during pregnancy rather than from gastrointestinal iron loss. A 2020 guideline from the American Gastroenterological Association notes that patients who place a high value on avoiding the small risk of endoscopy, particularly those who are young and might have other plausible reasons for iron deficiency anemia, and a low value on the very small risk of missing a gastrointestinal malignancy would reasonably select an initial course of iron replacement therapy and no initial investigation with bidirectional endoscopy (Option A).
Microcytosis with or without anemia is a manifestation of thalassemia. However, thalassemia is not the most likely explanation of this patient's anemia; the prominent anisopoikilocytosis and the decrease in the hemoglobin level and mean corpuscular volume that occurred during this patient's pregnancy are more suggestive of iron deficiency. Therefore, hemoglobin electrophoresis (Option D) would provide no additional diagnostic information.
Key Points
- Hypochromic and microcytic anemia, low reticulocyte count, and anisocytosis and poikilocytosis are characteristic of iron deficiency anemia.
- Frequent dosing (two or three times daily) of oral iron can lead to increased hepcidin production, which reduces iron absorption; a single daily or every-other-day dose of oral iron sulfate may be the best strategy.