MKSAP quiz: epigastric pain and daily heartburn
A 55-year-old white man has a several-year history of epigastric pain and daily heartburn without dysphagia or weight loss. He has tried over-the-counter antacids and, more recently, intermittent over-the-counter proton-pump inhibitors but still has breakthrough symptoms.
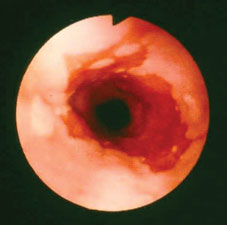
Physical examination is normal. Upper endoscopy is performed; findings from the distal esophagus are shown. Esophageal biopsy specimens show intestinal metaplasia. The patient is started on a once-daily proton-pump inhibitor with resolution of his symptoms.
Which of the following is the most appropriate long-term treatment for this patient?
A. Increase the proton-pump inhibitor to twice daily
B. Add an H2-receptor antagonist to his current regimen
C. Repeat upper endoscopy with biopsies to exclude dysplasia
D. Schedule laparoscopic fundoplication
Answer and Critique
The correct answer is C. Repeat upper endoscopy with biopsies to exclude dysplasia.
This patient has long-standing symptoms of gastroesophageal reflux disease. Upper endoscopy shows findings consistent with Barrett's esophagus, and esophageal biopsies show the presence of intestinal metaplasia, which confirms the diagnosis. Barrett's esophagus is a risk factor for development of adenocarcinoma of the esophagus. Because this patient has no dysplasia on initial endoscopy, current recommendations call for repeat endoscopy with biopsies to exclude dysplasia followed by surveillance endoscopy with esophageal biopsies every 3 years.
Changing to a high-dose (twice-daily) proton-pump inhibitor does not reliably cause regression of Barrett's esophagus. Adding an H2-receptor antagonist to his medical regimen is not needed because he has responded well to the proton-pump inhibitor. Laparoscopic fundoplication may be an option for his reflux symptoms but does not cause regression of Barrett's esophagus.
Key Points
- Barrett's esophagus is a risk factor for the development of esophageal adenocarcinoma.
- Patients with Barrett's esophagus without dysplasia should undergo surveillance upper endoscopy with esophageal biopsies every 3 years after the original diagnosis.

